💊Pharmacology for Nurses Unit 34 Review
34.1 Introduction to Diuretics
34.1 Introduction to Diuretics
Unit & Topic Study Guides
Introduction to Pharmacology
Drug Administration
Ethics and Safety in Pharmacology
Introduction to Homeostasis
Fluids, Electrolytes, Vitamins, and Minerals
Immune System and Inflammation Basics
Anti–infective Drugs
Cancer Therapy: Intro to Drugs and Treatment
Nervous System Basics for Nurses
Myasthenia Gravis & Alzheimer's Medications
Parkinson's and MS Drug Treatments
Anticonvulsants and Neurological Treatments
Psychopharmacologic Drugs
Pain Response Drugs
Substance Use Disorder Treatment Medications
Cardiovascular System Basics
Antidysrhythmic Drugs
Hypertension & Angina Medications
Heart Failure Drugs
Anticoagulants and Antiplatelets in Nursing
Lipid–Lowering Drugs
Cardiac Emergency and Shock Drugs
Respiratory System Basics for Nurses
Upper Respiratory Disorder Drugs
Lower Respiratory Disorder Drugs
Hypothalamic, Pituitary & Adrenal Drug Therapy
Thyroid & Parathyroid Medication
Diabetic Drugs
Digestive System Basics for Nurses
Gastrointestinal Disorder Drugs
Hyperacidity and Antiulcer Drugs
Weight Management Drugs
Renal and Urinary Systems Overview
Diuretic Drugs
Drugs for Urinary & Bladder Disorders
Reproductive Health Drugs
Transgender and Nonbinary Drugs
Ophthalmic Drugs
Otic Drugs
Diuretic Mechanisms and Effects
Diuretics are medications that increase urine output, helping manage fluid overload and high blood pressure. They work by targeting different segments of the nephron, and each class has distinct effects on electrolyte balance and fluid volume. Understanding where in the kidney each diuretic acts is the key to predicting its side effects and nursing considerations.
Loop, Thiazide, Potassium-Sparing, and Osmotic Diuretics
There are four major classes of diuretics, each acting on a different part of the nephron. The further "upstream" a diuretic acts (closer to the proximal tubule), the more water and solute it can pull out, which is why loop diuretics are the most potent.
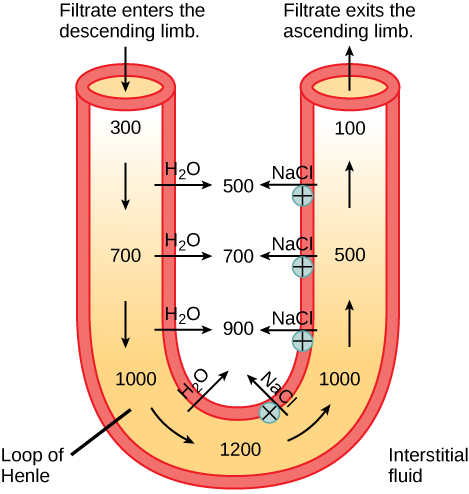
Loop diuretics (furosemide, bumetanide) act on the thick ascending limb of the loop of Henle. They inhibit the cotransporter (NKCC2), which blocks reabsorption of sodium, potassium, and chloride. The result is a large increase in water, sodium, potassium, and chloride excretion. These are the strongest diuretics and are often used in acute heart failure and severe edema.
Thiazide diuretics (hydrochlorothiazide, chlorthalidone) act on the distal convoluted tubule. They inhibit the cotransporter (NCC), decreasing reabsorption of sodium and chloride. They're less potent than loop diuretics but are first-line for chronic hypertension because of their steady, sustained effect on blood pressure.
Potassium-sparing diuretics act on the collecting duct and come in two subtypes:
- Aldosterone antagonists (spironolactone, eplerenone) block aldosterone receptors, which decreases sodium and water reabsorption while retaining potassium. Spironolactone is also used in heart failure for its mortality benefit.
- ENaC inhibitors (amiloride, triamterene) directly block the epithelial sodium channel (ENaC), producing a similar effect: increased sodium and water excretion with decreased potassium excretion.
Both subtypes are weak diuretics on their own and are often combined with loop or thiazide diuretics to offset potassium losses.
Osmotic diuretics (mannitol) work differently from the other classes. They act on the proximal tubule and descending limb of the loop of Henle by increasing the osmolarity of tubular fluid. Water stays in the tubule because it can't follow the osmotic gradient back into the blood. This increases excretion of water and electrolytes. Mannitol is primarily used to reduce intracranial or intraocular pressure, not for typical fluid overload.
Diuretic Effects on Fluid Volume and Electrolyte Balance
Each electrolyte shift matters clinically. Knowing which diuretic causes which imbalance helps you anticipate problems before they show up on labs.
Fluid volume: All diuretics increase urine output and decrease extracellular fluid volume. This reduced volume is what helps manage heart failure, hypertension, and edema.
Sodium: Most diuretics increase sodium excretion, lowering total body sodium. Since sodium holds onto water, decreased sodium levels reduce fluid retention and blood pressure. Watch for hyponatremia, especially with thiazides in older adults.
Potassium: This is the electrolyte you'll monitor most closely.
- Loop and thiazide diuretics increase potassium excretion, which can lead to hypokalemia (serum < 3.5 mEq/L). Symptoms include muscle weakness, cardiac dysrhythmias, and fatigue.
- Potassium-sparing diuretics decrease potassium excretion, which can lead to hyperkalemia (serum > 5.0 mEq/L). This is especially dangerous in patients with impaired kidney function.
Magnesium: Loop and thiazide diuretics also increase magnesium excretion, potentially causing hypomagnesemia. Low magnesium can worsen hypokalemia and make it harder to correct, so check both levels together.
Calcium: This is where loop and thiazide diuretics differ in a clinically useful way:
- Thiazides decrease calcium excretion, which can cause hypercalcemia but also makes them helpful for patients with osteoporosis or recurrent calcium kidney stones.
- Loop diuretics increase calcium excretion, which can cause hypocalcemia but can be used to treat acute hypercalcemia.

Key Laboratory Values for Monitoring Kidney Function and Diuretic Effectiveness
Before starting and throughout diuretic therapy, you need baseline and ongoing lab monitoring. Here are the values that matter most:
- Serum creatinine and BUN are markers of kidney function. Creatinine reflects the glomerular filtration rate (GFR), while BUN can rise with dehydration even if kidney function is stable. A rising creatinine during diuretic therapy may signal over-diuresis or worsening kidney function.
- Serum electrolytes (sodium, potassium, chloride, magnesium, calcium) should be checked regularly to detect imbalances caused by diuretic therapy. Potassium and magnesium are the most common concerns with loop and thiazide diuretics.
- Urine output is your real-time indicator of diuretic effectiveness. An expected increase confirms the drug is working. Oliguria (< 400 mL/day) or anuria suggests inadequate response or declining kidney function and should be reported promptly.
- Urine electrolytes (urinary sodium, potassium, chloride) help assess how well the diuretic is working and quantify electrolyte losses. A low urinary sodium despite diuretic therapy may indicate diuretic resistance.
- Glomerular filtration rate (GFR) is estimated using serum creatinine along with age and sex. It provides the best overall picture of kidney function and directly guides diuretic dosing. A declining GFR may require switching from a thiazide to a loop diuretic, since thiazides become less effective when GFR drops below approximately 30 mL/min.