🧠Intro to Brain and Behavior Unit 13 Review
13.2 Anxiety disorders
13.2 Anxiety disorders
Unit & Topic Study Guides
Nervous System Basics
Neurophysiology
Brain Structure and Organization
Sensory Systems
Motor Systems
Neurodevelopment
Learning and Memory
Emotion and Motivation
Language and Communication
Attention and Consciousness
Cognitive Functions
Brain Disorders: Developmental & Degenerative
Neurological & Psychiatric Disorders
Types of Anxiety Disorders
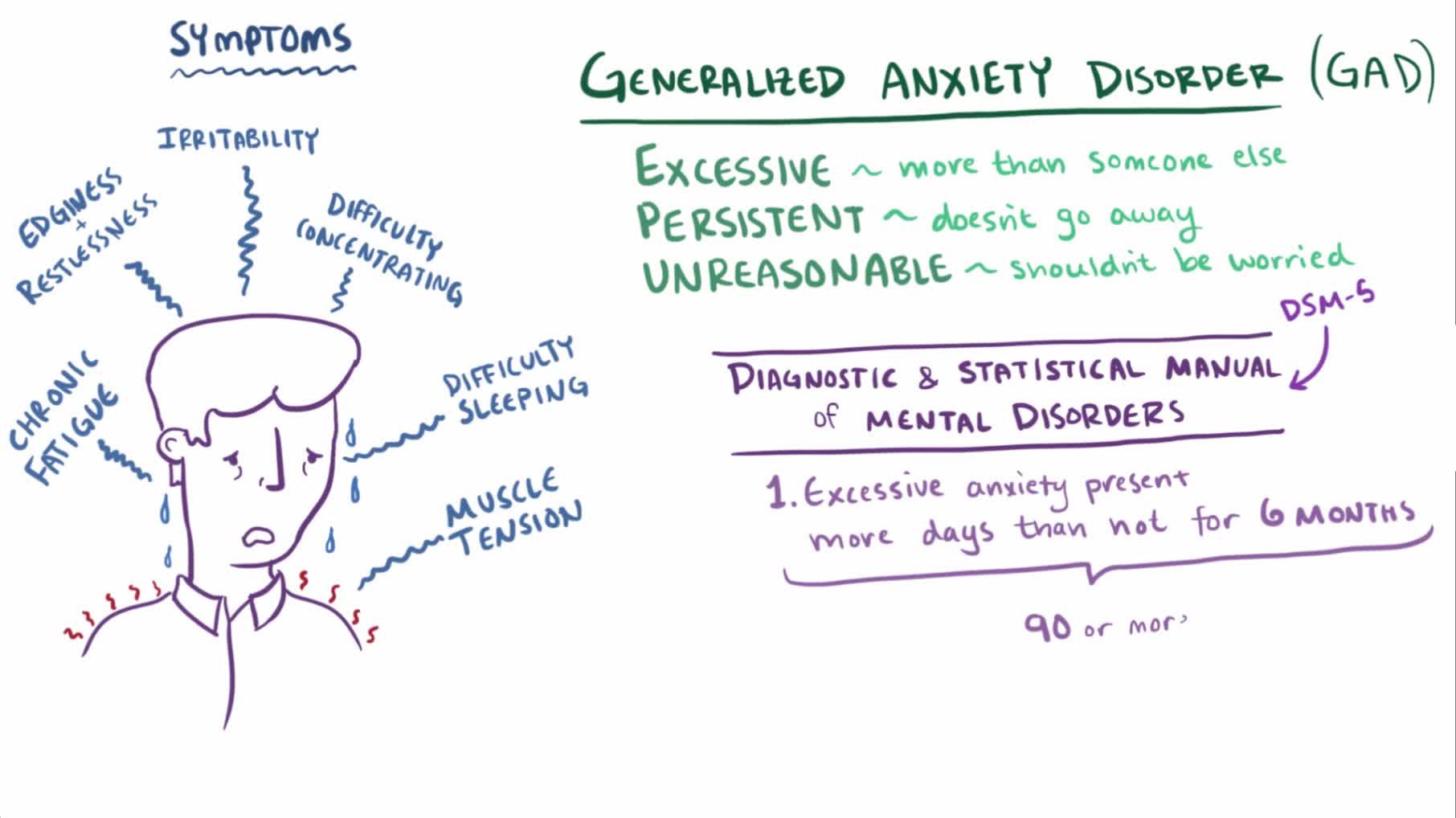
Generalized Anxiety Disorder (GAD) and Panic Disorder
Generalized anxiety disorder (GAD) is characterized by persistent, excessive worry about everyday things like health, finances, or work. The worry feels difficult to control and is out of proportion to the actual situation. GAD often comes with physical symptoms: restlessness, fatigue, muscle tension, difficulty concentrating, and sleep disturbances.
Panic disorder involves recurrent, unexpected panic attacks. These are sudden surges of intense fear or discomfort accompanied by physical symptoms like heart palpitations, trembling, sweating, and shortness of breath. A key feature is that the person develops persistent concern about having future attacks, which can itself become a source of anxiety.
Specific Phobias and Social Anxiety Disorder (SAD)
Specific phobias are marked by intense, irrational fear of a particular object or situation, such as heights, spiders, or enclosed spaces. The fear is disproportionate to the actual danger. People with specific phobias develop avoidance behaviors that can significantly interfere with daily life. For example, someone with a phobia of flying might turn down job opportunities that require travel.
Social anxiety disorder (SAD) involves a persistent, intense fear of social or performance situations. It's driven by concerns about being judged, embarrassed, or humiliated by others. This goes well beyond ordinary shyness. People with SAD may avoid speaking in class, eating in public, or attending social gatherings, and the avoidance causes real impairment.
Agoraphobia and Separation Anxiety Disorder
Agoraphobia is a fear of being in situations where escape might be difficult or help might not be available if anxiety symptoms occur. This often leads to avoidance of public places, crowds, public transportation, or traveling alone. In severe cases, individuals may become housebound.
Separation anxiety disorder involves excessive fear or anxiety about being separated from home or attachment figures. While more commonly diagnosed in children (where it can lead to school refusal, nightmares, and physical complaints like stomachaches), it can also occur in adults. Symptoms appear when separation occurs or is even anticipated.

Anxiety Disorder Mechanisms
Biological Factors
Genetic factors contribute to anxiety vulnerability. Twin studies show higher concordance rates among monozygotic (identical) twins compared to dizygotic (fraternal) twins, indicating a heritable component. No single "anxiety gene" has been identified; rather, multiple genes likely contribute to risk.
Neurotransmitter imbalances are implicated in anxiety disorders, particularly involving three systems:
- Serotonin and norepinephrine: dysregulation in these systems is linked to heightened anxiety and mood disturbance
- GABA (gamma-aminobutyric acid): the brain's primary inhibitory neurotransmitter. Reduced GABA activity means less inhibition of neural circuits, which can leave the brain in an overexcited, anxious state
Structural and functional abnormalities have been observed in brain regions involved in threat processing. The amygdala (which detects threats and triggers fear responses) tends to show hyperactivity in anxiety disorders. The prefrontal cortex (involved in regulating emotional responses) may show reduced activity, meaning the brain's "brake" on fear is weaker. The hippocampus (important for contextual memory) can also be affected, making it harder to distinguish safe contexts from threatening ones.
Psychological Factors
Classical conditioning can explain how specific phobias develop. A previously neutral stimulus (like a dog) becomes associated with a fear response after being paired with an aversive event (like a dog bite). After that pairing, the dog alone triggers a conditioned fear response, even in safe situations.
Cognitive biases help maintain and worsen anxiety once it develops:
- Attentional bias: selectively noticing threat-related information in the environment
- Interpretive bias: perceiving ambiguous situations as threatening (e.g., assuming a friend's short text message means they're angry)
These biases reinforce a cycle of hypervigilance and avoidance.
Early life experiences also shape anxiety vulnerability. Adverse childhood events, insecure attachment styles, or overprotective parenting can lead to maladaptive coping strategies and patterns of emotional processing that increase the risk of developing an anxiety disorder later.
Normal vs. Pathological Anxiety
Not all anxiety is a disorder. Normal anxiety is actually adaptive. It motivates you to study for an exam, avoid a dangerous situation, or prepare for a job interview.
Here's how to distinguish the two:
| Feature | Normal Anxiety | Pathological Anxiety |
|---|---|---|
| Proportion | Matches the situation | Disproportionate to actual threat |
| Duration | Time-limited; fades when stressor passes | Prolonged; persists even without a clear stressor |
| Functioning | Does not significantly impair daily life | Causes significant distress and impairment in social, occupational, or other areas |
| Response to coping | Responsive to reassurance and coping strategies | Persists despite attempts at rational thinking or relaxation |
| Behavior | May prompt helpful preparation | Leads to avoidance behaviors that reduce quality of life |
The core distinction comes down to intensity, duration, and functional impairment. When anxiety becomes persistent, excessive, and irrational to the point that it disrupts someone's ability to live their life, it crosses into pathological territory.
Treatment for Anxiety Disorders
Cognitive-Behavioral Therapy (CBT) and Exposure Therapy
Cognitive-behavioral therapy (CBT) is one of the most well-supported treatments for anxiety disorders. It works by helping individuals identify and modify the maladaptive thoughts and behaviors that maintain their anxiety.
Exposure therapy is a key component of CBT for anxiety. The process works like this:
- The therapist and patient build a fear hierarchy, ranking feared stimuli from least to most anxiety-provoking
- The patient is gradually and systematically exposed to these feared stimuli, starting with the least threatening
- Through repeated exposure in a controlled environment, the anxiety response weakens over time (a process called extinction)
- Avoidance behaviors decrease as the patient learns that the feared outcome doesn't occur or is manageable
Relaxation Techniques and Medication
Relaxation techniques can help manage the physiological symptoms of anxiety. These include deep breathing exercises, progressive muscle relaxation, and mindfulness meditation. They work by activating the parasympathetic nervous system, promoting calm and emotional regulation.
On the medication side, several classes of drugs are used:
- SSRIs (selective serotonin reuptake inhibitors) and SNRIs (serotonin-norepinephrine reuptake inhibitors) are first-line medications for anxiety disorders. They target neurotransmitter imbalances but take several weeks to reach full effectiveness.
- Benzodiazepines are fast-acting anti-anxiety medications that enhance GABA activity, providing rapid relief from acute anxiety. However, they carry a risk of dependence and are typically prescribed only for short-term use.
Combination Therapy and Treatment Effectiveness
A combination of psychotherapy (usually CBT) and medication is often the most effective approach. This targets both the psychological factors (maladaptive thoughts and behaviors) and the biological factors (neurotransmitter imbalances) contributing to the disorder.
Treatment effectiveness depends on several factors:
- Severity and duration of symptoms
- Presence of co-occurring mental health conditions
- Patient adherence to the treatment plan
- The quality of the therapeutic alliance between patient and provider