🤔Cognitive Psychology Unit 15 Review
15.2 Neuroplasticity and Cognitive Processes
15.2 Neuroplasticity and Cognitive Processes
Unit & Topic Study Guides
Introduction to Cognitive Psychology
History of Cognitive Psychology
Research Methods in Cognitive Psychology
Perception
Attention
Short–term and Working Memory
Long–term Memory
Knowledge Representation
Language Processing
Problem Solving
Reasoning and Decision Making
Cognitive Development
Intelligence
Consciousness
Cognitive Neuroscience
Emotion and Cognition
Social Cognition
Cognitive Biases and Heuristics
Cognitive Disorders
Neuroplasticity and Cognitive Processes
Neuroplasticity is the brain's ability to reorganize its structure and function in response to experience, learning, and injury. It underpins nearly every cognitive process covered in this course, from memory formation to language acquisition, and explains how the brain remains adaptable well beyond early development.
This section covers the core mechanisms behind neuroplasticity, the evidence that experience physically reshapes the brain, and how researchers are applying these principles in rehabilitation, education, and cognitive training.
Neuroplasticity Fundamentals
Neuroplasticity in cognitive development
The brain doesn't stop changing after childhood. Neuroplasticity allows neural connections to form, strengthen, or weaken across the entire lifespan, from infancy through old age. That said, the type and degree of plasticity shift over time.
During childhood, plasticity is at its peak. New neural pathways form rapidly, which is why children pick up languages and motor skills (walking, writing, tying shoes) so quickly. In adulthood, plasticity continues but tends to be more targeted. Learning a new language at 30, for instance, still creates measurable changes in the brain, but the process is slower and relies on somewhat different mechanisms than it would at age 5.
Two broad categories of neuroplasticity matter here:
- Structural plasticity refers to physical changes in the brain, such as growth of new dendrites, increased gray matter volume in specific regions, or the formation of entirely new neurons.
- Functional plasticity involves changes in how the brain operates without necessarily altering its physical structure. For example, after damage to one region, neighboring areas may take over the lost function.
Both types work together to support learning, memory, and recovery from injury.

Mechanisms of synaptic plasticity
At the cellular level, plasticity comes down to how synapses (the junctions between neurons) get stronger or weaker over time. Four key mechanisms drive this:
- Long-term potentiation (LTP) strengthens synaptic connections when two neurons are repeatedly activated together. This is the primary cellular mechanism behind memory formation. When you study a fact and successfully recall it later, LTP has made that neural pathway more efficient at transmitting signals.
- Long-term depression (LTD) does the opposite: it weakens synaptic connections that are rarely used. This isn't a failure of the brain. It's selective pruning that helps you discard irrelevant information and keeps neural networks efficient.
- Hebbian learning is the principle often summarized as "neurons that fire together, wire together." When two neurons are consistently activated at the same time, the connection between them strengthens. This is how habits form and how associations between concepts get built (like automatically linking the smell of coffee with your morning routine).
- Synaptic scaling is a homeostatic mechanism that keeps the whole network stable. If a group of synapses becomes too strong (risking overexcitation), synaptic scaling dials them down proportionally. If they become too weak, it boosts them. Think of it as the brain's way of preventing runaway activity while still allowing learning to occur.
These mechanisms collectively support:
- Memory formation and consolidation
- Learning and skill acquisition
- Attention and perceptual adaptation
Applications and Evidence
Evidence for experience-dependent plasticity
A core claim of neuroplasticity research is that specific experiences produce measurable changes in the brain. The evidence for this comes from several converging lines of research:
- Neuroimaging studies using fMRI and PET scans show that learning tasks increase activation in relevant brain areas. For example, people learning a second language show heightened activity in Broca's and Wernicke's areas during the training period.
- Structural MRI reveals that skill acquisition correlates with changes in gray matter volume. The most famous example: London taxi drivers, who must memorize thousands of street routes, have significantly larger posterior hippocampi than control subjects. The longer they've been driving, the larger the difference.
- Longitudinal studies track the same individuals over time and show that sustained training reshapes brain structure. Professional musicians, for instance, develop an enlarged auditory cortex compared to non-musicians, and the degree of enlargement correlates with years of practice.
- Brain injury case studies demonstrate functional reorganization. After left-hemisphere stroke damage, some patients gradually shift language processing to the right hemisphere, a clear example of functional plasticity compensating for structural damage.
- Sensory substitution experiments show that brain regions can be repurposed for entirely different inputs. In congenitally blind individuals, the visual cortex processes tactile information (such as Braille reading), demonstrating that cortical function is not rigidly predetermined.
- Critical periods are windows of heightened plasticity during development. Language acquisition is the classic example: children exposed to language before roughly age 5-7 acquire it with native-level fluency far more easily than older learners. After the critical period closes, plasticity for that function decreases (though it doesn't disappear entirely).
- Adult neurogenesis provides evidence that new neurons continue to form in specific regions throughout life, particularly the hippocampus (involved in memory) and the olfactory bulb. This challenges the old assumption that adults are stuck with the neurons they have.
Applications of neuroplasticity
Researchers and clinicians have translated these findings into practical interventions:
- Cognitive training programs use structured exercises (often called "brain games") to target specific functions like working memory. Results are mixed: people generally improve on the trained tasks, but whether those gains transfer to real-world cognitive performance remains debated.
- Neurorehabilitation applies plasticity principles to help patients recover function after brain injury or stroke. Constraint-induced movement therapy is a well-supported example: by restraining the unaffected limb, the therapy forces the brain to rebuild motor pathways for the affected side.
- Neurofeedback gives patients real-time information about their own brain activity (typically via EEG), allowing them to learn self-regulation strategies. It has shown promise for ADHD and anxiety disorders, though the evidence base is still developing.
- Transcranial magnetic stimulation (TMS) uses magnetic pulses to non-invasively stimulate or inhibit specific brain regions. It's FDA-approved for treatment-resistant depression and is being explored for other conditions.
- Educational interventions informed by neuroscience design learning environments that take advantage of how plasticity works. Techniques like spaced repetition (distributing study sessions over time) and active recall (testing yourself rather than re-reading) directly leverage LTP and Hebbian learning to strengthen memory traces more effectively.
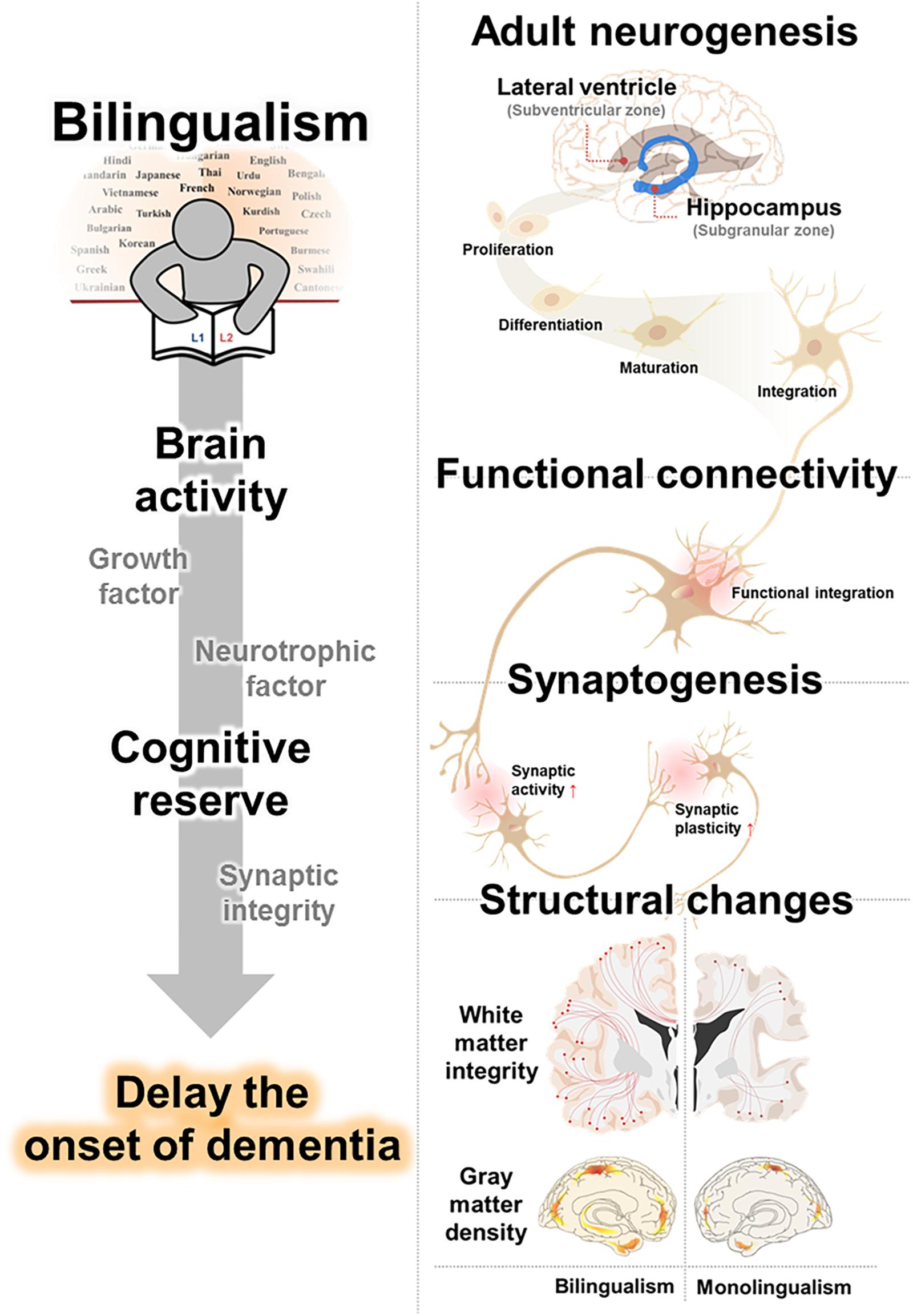
- Cognitive reserve hypothesis suggests that a lifetime of intellectual engagement (learning new skills, bilingualism, complex hobbies) builds a buffer against age-related cognitive decline. The idea is that a richly connected brain has more alternative neural pathways to fall back on when some connections deteriorate. This doesn't prevent neurodegeneration, but it may delay the point at which cognitive symptoms become noticeable.